Acne is a common and unwanted response to hormonal replacement therapy - specifically, testosterone - so as a long-term sufferer of chronic acne, I put together a guide to help others battle this unwanted skin condition. I have been to quite a few different dermatologists over the years and done quite a bit of research on the subject, so this is pretty much a comprehensive and cross-refered thesis on everything I know about acne.
Identifying your acne: Before we get into it, it's helpful to know your enemy and identify what type of acne you're experiencing.
Non-inflammatory acne:
In the first category, you have your non-inflammatory acne; blackheads(open comedones) and whiteheads(closed comedones). Blackheads and whiteheads are primarily caused by a build-up of sebum and dead skin cells within or at the entrance of the pore. Blackheads are essentially little waxy plugs at the opening of the pore that can be squeezed out fairly painlessly. They're not inflamed and typically won't bleed when you squeeze them unless you really manage to reef on them. The distinction between blackheads and whiteheads is that with blackheads, the top of the pore remains open, while with whiteheads, the top of the pore is closed. Here is a cross-section illustrating the difference between blackheads and whiteheads. Non-inflammatory acne is the most benign of all of them, but it's still not fun and can progress to inflammatory acne.
Inflammatory Acne:
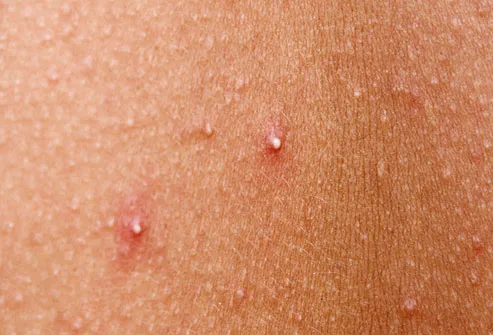
The three main types of inflammatory acne are papules, pustules, and cysts (nodules). The key difference between inflammation and non-inflammatory acne is that with inflammatory acne, the clogged pores have backed up and pressurized to the point where the cell walls have ruptured. Papules and pustules are the inflamed and raised bumps that will often weep pus and blood when squeezed. The third type of inflammatory acne, cysts, or nodules, occur when the pore clogs deep beneath the surface of the skin and entrance of the pore. This type of acne forms deep, hard, painful bumps that may not have any visible heads, and can sometimes grow to the size of a penny or larger. Cystic acne nodes can be circular, oblong, or amorphously shaped. Extreme cystic acne breakouts can make it painful to eat, talk, or smile when the skin is stretched too tightly over the nodules. Never attempt to pop a nodule as the pressure is far more likely to rupture your pores further than it is to force the pus out through the head.
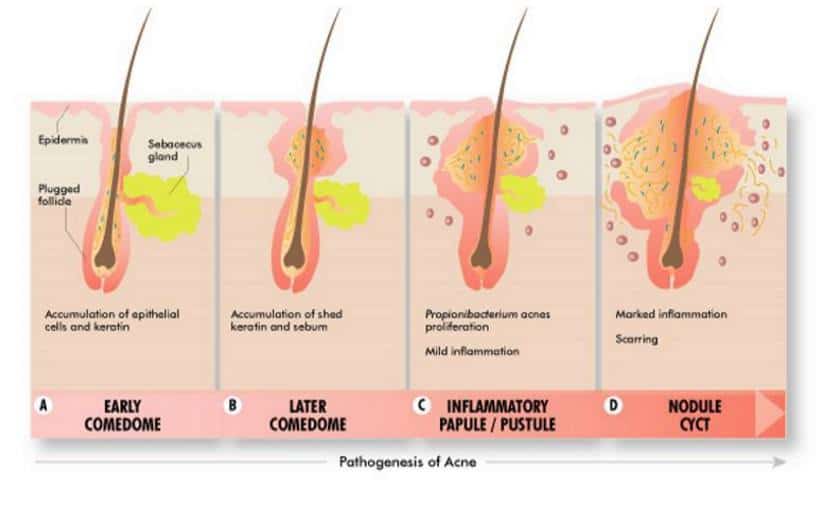
Here is a cute little cross-section that shows the differences between inflammatory acne. It's important to note that acne does not always progress linearly - you can develop a cystic nodule without ever forming a blackhead, and you can have a blackhead that will never turn into a cyst.
Inflammatory acne is also caused by a build-up of dead skin cells and sebum, but another factor comes into play as well; p. acnes bacteria. When seperated, both sebum and p. acnes aren't particularly problematic and are healthy at appropriate levels. However, when combined in an environment low in oxygen, such as your clogged pore, they catalyze. The p. acnes bacteria transforms relatively harmless, oily sebum into inflammatory fatty acids. The reason why puberty and hormonal changes cause acne is because these changes trigger the production of excess sebum in the skin, increasing the likelihood of clogged pores which snowballs into an infestation of p. acnes bacteria. This is further exasperated when white blood cells flood the area to fight the infection, further clogging the pores. P. acnes is present in all forms of acne and on the surface of your skin at pretty much any given time, however it becomes especially problematic with inflammatory acne.
Identifying the source of your acne: Now that we know the causes of acne, we know that it can develop pretty much anywhere for any reason. However, if you're breaking out consistently in a specific area, it can give you a bit more insight into exactly what is causing it.
Hairline breakouts are probably a result of a bothersome hair product. Try switching up your haircare regime.
Breakouts on your forehead and nose are probably a result of excessive oil buildup.
Cheek breakouts are also due to excess oil, but could also be exacerbated by regular contact with a dirty phone screen, dirty pillowcase, etc.
Acne on and under your jawline and around your shoulders and back are indicative of a hormonal breakout. Back and shoulder breakouts can also be caused by dirty, tight clothing - like binders. Obviously for some people, like me, not wearing a binder isn't an option, so if body acne is a problem around the area you bind, try to keep your binder as clean and fresh as possible - wash it frequently and invest in a few more if you can so you can rotate them.
Treating Acne:
Hopefully by now you know what type of acne you have and what is causing it, so let's move on to solutions.
This guide primarily focuses on inflammatory acne - specifically, hormonal acne - but many of these tips and resources can be applied to other types of acne as well.
When treating inflammatory acne, most dermatologist recommended treatments primarily target the p. acnes bacteria, with a secondary emphasis on external oil reduction and exfoliation.
Step 1: kill the bacteria.
The most common and generally most effective over-the-counter remedy is going to be a topical benzoyl peroxide cream, similar to this. I have noticed some face and body washes popping up here and there that claim to have benzoyl peroxide as an active ingredient - I haven't tried them so I can't speak to their effectiveness, but it's my understanding that benzoyl peroxide needs to applied like a lotion and pretty much left alone so it has the chance to really sink in and penetrate through to the pores to have the chance to work - but I'm not sure how those washes are formulated.
From my experience, benzoyl peroxide is effective to a degree. It's not likely to get rid of your acne overnight or prevent it entirely - some people may get lucky, but I wouldn't gamble on it being a one-step cure-all. If you want to go straight for the jugular, you can set up an appointment with a dermatologist and they'll likely prescribe you an antibiotic formulated to kill p. acnes bacteria. This is an extremely effective option for bad-flare ups and temporary hormonal imbalances.
Step 2: Reduce oil on your skin surface.
There is a balance to strike with this, because too harsh of a routine will dry your skin out excessively which can actually cause more acne - which is the opposite result intended. If you're using benzoyl peroxide to kill off those nasty little bacteria, keep in mind that has a drying effect on your skin as well, so try not to push things too far with your face-washing regime. My dermatologists have consistently recommended Cetaphil (or CeraVe) Gentle Skin Cleanser. I pair this with a gentle exfoliating pad to scrub away any dead skin cells on the surface. Personally, I avoid face washes with "exfoliating beads" because many of them contain microplastics which are too small to be caught by some municipal water treatment plants and end up getting deposited into natural water sources. If you're not sure if you're using personal hygiene products that contain microplastics, check the ingredients list for polyethylene, polypropylene, polymethyl methacrylate, nylon, polyurethane, and acrylates copolymer.
If you can use them without drying your skin excessively, you can also supplement your face wash with toners. I personally prefer glycolic acid based toners over toners with salicylic acid because it has less of a drying effect while still promoting a good turnover of dead skin. I use a glycolic acid toner by Bevel, personally.
Step 3: Moisturize.
Moisturizer is an important part of keeping a healthy skin balance and preventing acne. You'll want a lotion that is lightweight, oil-free, and fragrance free so that you can keep your skin moisturized without globbing on a bunch of other unnecessary ingredients that will clog your pores. My dermatologists have recommended a Cetaphil facial lotion with SPF for sun protection during the day if you will be spending time outside. There's also a CeraVe PM formula without SPF protection for night use, or if you spend most of your time indoors.
General notes:
A good rule of thumb is that if something does not need to be in your face, don't put it on your face. You want your routine to be concise and effective - bigger and more is not always better. It's frustrating when acne takes a while to clear, and it's tempting to abandon a routine that doesn't seem to be working, or to try that cool looking product that you happened to see, but stability in your routine is going to help you the most in the long run. Trust the process.
That rule of thumb applies to things touching your face as well! Avoid picking at scabs (do as I say, not as I do) and touching your face. I'm a side sleeper and I noticed thar my acne was consistently worse on the side where I pillow my head on my elbow - I can't easily change the position I sleep in, so I asked my grandmother to make me a small, pillow-case sized blanket so I can at least lay that between my face and my arm when I'm sleeping so I don't have that consistent skin-to-skin contact every night, and it helped.
And on that note, wash your sheets and pillowcase religiously. If I could feasibility have a fresh pillowcase every night, I absolutely would. If you get your eight hours of sleep every night, you spend 56 hours per week mashing your head into your pillow. Keeping that surface clean of old facial oil and sloughed off dead skin cells can really make a difference.
I've heard some people say that it's also beneficial to finish off your showers or face-washing time with a good douse if cold water to close up your pores. I believe it's supposed to be good for your hair as well - I however, will not do that because life is miserable enough without throwing cold showers into the mix. /s
Chronic Acne Solutions: However, for some unlucky people (like me), even this is not enough. If is cystic, it's not likely to respond well to a basic skin care regime. Unfortunately, cystic acne often requires a visit to your dermatologist to cure. If antibiotics fail to clear it up, or if it keeps recurring despite antibiotic treatment, you will likely need to take a course of Accutaine (isotretinoin). Isotretinoin is a retinoid that treats acne by altering the DNA transcription of your skin cells. It decreases the size and output of your sebaceous glands and modifies the skin cells that get sloughed off into the glands by making them less likely to cause blockages. In addition, it targets p. acnes bacteria. Isotretinoin is a very powerful three-pronged attack that is designed to end problematic acne once and for all. If antibiotics are going for the jugular, isotretinoin is dropping a bomb on it and walking away. But isotretinoin is a last-resort treatment with some potentially serious side effects. First of all, it's hard on your liver. If you are already on HRT, your labs have to be consistently in the clear before isotretinoin can be considered. Additionally, you will need routine lab work while you are on isotretinoin (typically around 6-8 months) to ensure your levels stay clear. Isotretinoin had been confirmed to cause serious birth defects. If you have intact female anatomy and disclose that to your dermatologist, you will be required to take a barrage of pregnancy tests on a routine basis to keep your prescription, which is obviously very dysphoric. And isotretinoin is expensive - one month, without insurance, is around $500-600 USD. With GoodRx, I pay about $120 per month, but that's still a substantial cost, excluding the cost of seeing a dermatologist and having the required labs done.
Hopefully you will never need isotretinoin to cure your acne, but it is an option to consider if all else fails. I'm currently on my fourth month of isotretinoin and I'm simply relieved to have clear skin for the first time since I was a kid - and I'm 27. Frankly, I wish I had started it years ago, because while my acne is gone now, I still have some fairly bad scarring from it running rampant for over a decade - but scarring is treatable as well, and that's an adventure I'll get into once this acne is gone for good.
Conclusion:
I'm not a dermatologist, just a patient that's been around the block with this stuff - I prefer to know my enemy and have done a lot of research over the years, but if I am wrong on anything or missed any important points, please feel free to comment.
References: 1, 2, 3, 4, 5, 6
Hopefully all that helps!
Acne is a common and unwanted response to hormonal replacement therapy - specifically, testosterone - so as a long-term sufferer of chronic acne, I put together a guide to help others battle this unwanted skin condition. I have been to quite a few different dermatologists over the years and done quite a bit of research on the subject, so this is pretty much a comprehensive and cross-refered thesis on everything I know about acne.Identifying your acne: Before we get into it, it's helpful to know your enemy and identify what type of acne you're experiencing.Non-inflammatory acne:In the first category, you have your non-inflammatory acne; blackheads(open comedones) and whiteheads(closed comedones). Blackheads and whiteheads are primarily caused by a build-up of sebum and dead skin cells within or at the entrance of the pore. Blackheads are essentially little waxy plugs at the opening of the pore that can be squeezed out fairly painlessly. They're not inflamed and typically won't bleed when you squeeze them unless you really manage to reef on them. The distinction between blackheads and whiteheads is that with blackheads, the top of the pore remains open, while with whiteheads, the top of the pore is closed. Here is a cross-section illustrating the difference between blackheads and whiteheads. Non-inflammatory acne is the most benign of all of them, but it's still not fun and can progress to inflammatory acne.Inflammatory Acne:The three main types of inflammatory acne are papules, pustules, and cysts (nodules). The key difference between inflammation and non-inflammatory acne is that with inflammatory acne, the clogged pores have backed up and pressurized to the point where the cell walls have ruptured. Papules and pustules are the inflamed and raised bumps that will often weep pus and blood when squeezed. The third type of inflammatory acne, cysts, or nodules, occur when the pore clogs deep beneath the surface of the skin and entrance of the pore. This type of acne forms deep, hard, painful bumps that may not have any visible heads, and can sometimes grow to the size of a penny or larger. Cystic acne nodes can be circular, oblong, or amorphously shaped. Extreme cystic acne breakouts can make it painful to eat, talk, or smile when the skin is stretched too tightly over the nodules. Never attempt to pop a nodule as the pressure is far more likely to rupture your pores further than it is to force the pus out through the head.Here is a cute little cross-section that shows the differences between inflammatory acne. It's important to note that acne does not always progress linearly - you can develop a cystic nodule without ever forming a blackhead, and you can have a blackhead that will never turn into a cyst.Inflammatory acne is also caused by a build-up of dead skin cells and sebum, but another factor comes into play as well; p. acnes bacteria. When seperated, both sebum and p. acnes aren't particularly problematic and are healthy at appropriate levels. However, when combined in an environment low in oxygen, such as your clogged pore, they catalyze. The p. acnes bacteria transforms relatively harmless, oily sebum into inflammatory fatty acids. The reason why puberty and hormonal changes cause acne is because these changes trigger the production of excess sebum in the skin, increasing the likelihood of clogged pores which snowballs into an infestation of p. acnes bacteria. This is further exasperated when white blood cells flood the area to fight the infection, further clogging the pores. P. acnes is present in all forms of acne and on the surface of your skin at pretty much any given time, however it becomes especially problematic with inflammatory acne.Identifying the source of your acne: Now that we know the causes of acne, we know that it can develop pretty much anywhere for any reason. However, if you're breaking out consistently in a specific area, it can give you a bit more insight into exactly what is causing it.Hairline breakouts are probably a result of a bothersome hair product. Try switching up your haircare regime.Breakouts on your forehead and nose are probably a result of excessive oil buildup.Cheek breakouts are also due to excess oil, but could also be exacerbated by regular contact with a dirty phone screen, dirty pillowcase, etc.Acne on and under your jawline and around your shoulders and back are indicative of a hormonal breakout. Back and shoulder breakouts can also be caused by dirty, tight clothing - like binders. Obviously for some people, like me, not wearing a binder isn't an option, so if body acne is a problem around the area you bind, try to keep your binder as clean and fresh as possible - wash it frequently and invest in a few more if you can so you can rotate them.Treating Acne:Hopefully by now you know what type of acne you have and what is causing it, so let's move on to solutions.This guide primarily focuses on inflammatory acne - specifically, hormonal acne - but many of these tips and resources can be applied to other types of acne as well.When treating inflammatory acne, most dermatologist recommended treatments primarily target the p. acnes bacteria, with a secondary emphasis on external oil reduction and exfoliation.Step 1: kill the bacteria.The most common and generally most effective over-the-counter remedy is going to be a topical benzoyl peroxide cream, similar to this. I have noticed some face and body washes popping up here and there that claim to have benzoyl peroxide as an active ingredient - I haven't tried them so I can't speak to their effectiveness, but it's my understanding that benzoyl peroxide needs to applied like a lotion and pretty much left alone so it has the chance to really sink in and penetrate through to the pores to have the chance to work - but I'm not sure how those washes are formulated.From my experience, benzoyl peroxide is effective to a degree. It's not likely to get rid of your acne overnight or prevent it entirely - some people may get lucky, but I wouldn't gamble on it being a one-step cure-all. If you want to go straight for the jugular, you can set up an appointment with a dermatologist and they'll likely prescribe you an antibiotic formulated to kill p. acnes bacteria. This is an extremely effective option for bad-flare ups and temporary hormonal imbalances.Step 2: Reduce oil on your skin surface.There is a balance to strike with this, because too harsh of a routine will dry your skin out excessively which can actually cause more acne - which is the opposite result intended. If you're using benzoyl peroxide to kill off those nasty little bacteria, keep in mind that has a drying effect on your skin as well, so try not to push things too far with your face-washing regime. My dermatologists have consistently recommended Cetaphil (or CeraVe) Gentle Skin Cleanser. I pair this with a gentle exfoliating pad to scrub away any dead skin cells on the surface. Personally, I avoid face washes with "exfoliating beads" because many of them contain microplastics which are too small to be caught by some municipal water treatment plants and end up getting deposited into natural water sources. If you're not sure if you're using personal hygiene products that contain microplastics, check the ingredients list for polyethylene, polypropylene, polymethyl methacrylate, nylon, polyurethane, and acrylates copolymer.If you can use them without drying your skin excessively, you can also supplement your face wash with toners. I personally prefer glycolic acid based toners over toners with salicylic acid because it has less of a drying effect while still promoting a good turnover of dead skin. I use a glycolic acid toner by Bevel, personally.Step 3: Moisturize.Moisturizer is an important part of keeping a healthy skin balance and preventing acne. You'll want a lotion that is lightweight, oil-free, and fragrance free so that you can keep your skin moisturized without globbing on a bunch of other unnecessary ingredients that will clog your pores. My dermatologists have recommended a Cetaphil facial lotion with SPF for sun protection during the day if you will be spending time outside. There's also a CeraVe PM formula without SPF protection for night use, or if you spend most of your time indoors.General notes:A good rule of thumb is that if something does not need to be in your face, don't put it on your face. You want your routine to be concise and effective - bigger and more is not always better. It's frustrating when acne takes a while to clear, and it's tempting to abandon a routine that doesn't seem to be working, or to try that cool looking product that you happened to see, but stability in your routine is going to help you the most in the long run. Trust the process.That rule of thumb applies to things touching your face as well! Avoid picking at scabs (do as I say, not as I do) and touching your face. I'm a side sleeper and I noticed thar my acne was consistently worse on the side where I pillow my head on my elbow - I can't easily change the position I sleep in, so I asked my grandmother to make me a small, pillow-case sized blanket so I can at least lay that between my face and my arm when I'm sleeping so I don't have that consistent skin-to-skin contact every night, and it helped.And on that note, wash your sheets and pillowcase religiously. If I could feasibility have a fresh pillowcase every night, I absolutely would. If you get your eight hours of sleep every night, you spend 56 hours per week mashing your head into your pillow. Keeping that surface clean of old facial oil and sloughed off dead skin cells can really make a difference.I've heard some people say that it's also beneficial to finish off your showers or face-washing time with a good douse if cold water to close up your pores. I believe it's supposed to be good for your hair as well - I however, will not do that because life is miserable enough without throwing cold showers into the mix. /sChronic Acne Solutions: However, for some unlucky people (like me), even this is not enough. If is cystic, it's not likely to respond well to a basic skin care regime. Unfortunately, cystic acne often requires a visit to your dermatologist to cure. If antibiotics fail to clear it up, or if it keeps recurring despite antibiotic treatment, you will likely need to take a course of Accutaine (isotretinoin). Isotretinoin is a retinoid that treats acne by altering the DNA transcription of your skin cells. It decreases the size and output of your sebaceous glands and modifies the skin cells that get sloughed off into the glands by making them less likely to cause blockages. In addition, it targets p. acnes bacteria. Isotretinoin is a very powerful three-pronged attack that is designed to end problematic acne once and for all. If antibiotics are going for the jugular, isotretinoin is dropping a bomb on it and walking away. But isotretinoin is a last-resort treatment with some potentially serious side effects. First of all, it's hard on your liver. If you are already on HRT, your labs have to be consistently in the clear before isotretinoin can be considered. Additionally, you will need routine lab work while you are on isotretinoin (typically around 6-8 months) to ensure your levels stay clear. Isotretinoin had been confirmed to cause serious birth defects. If you have intact female anatomy and disclose that to your dermatologist, you will be required to take a barrage of pregnancy tests on a routine basis to keep your prescription, which is obviously very dysphoric. And isotretinoin is expensive - one month, without insurance, is around $500-600 USD. With GoodRx, I pay about $120 per month, but that's still a substantial cost, excluding the cost of seeing a dermatologist and having the required labs done.Hopefully you will never need isotretinoin to cure your acne, but it is an option to consider if all else fails. I'm currently on my fourth month of isotretinoin and I'm simply relieved to have clear skin for the first time since I was a kid - and I'm 27. Frankly, I wish I had started it years ago, because while my acne is gone now, I still have some fairly bad scarring from it running rampant for over a decade - but scarring is treatable as well, and that's an adventure I'll get into once this acne is gone for good.Conclusion:I'm not a dermatologist, just a patient that's been around the block with this stuff - I prefer to know my enemy and have done a lot of research over the years, but if I am wrong on anything or missed any important points, please feel free to comment.References: 1, 2, 3, 4, 5, 6Hopefully all that helps! https://ift.tt/eA8V8J https://ift.tt/2ZQlvIS
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comments
Post a Comment